subhanallah! there is no impossible things to Allah. Allah Maha Berkuasa atas segala yang berlaku.
have you ever heard about TRAP-twin reversed arterial perfusion? it is a condition occurs in twin pregnancy where one twin supplies blood and nutrition to the other twin which is already dead.
this was the first time i heard about the phenomenon.
emm...kalau dalam bahasa melayu mungkin dipanggil "kembar pengepam darah". kes ni berlaku 1 dalam 35000 pregnancies. dan yang satu tu pernah ada di wad kuning dekat sini.
kisahnya macam ni...
TRAP ni ialah satu komplikasi yang sangatlah jarang berlaku di kalangan ibu yang mengandung kembar. ia melibatkan satu kembar yang ada kecatatan dari segi struktur dan tidak boleh survive manakala kembar yang satu lagi adalah normal dan bertindak sebagai pembekal darah dan makanan kepada pasangan kembarnya tu.
nak tahu lebih lanjut, boleh la google2. macam2 ada.
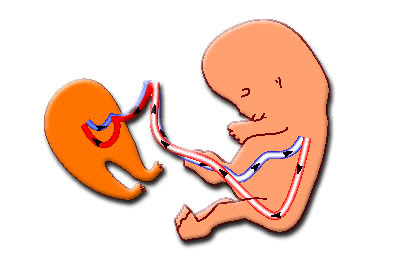
Ini nak menunjukkan bagaimana TRAP terjadi. darah dan makanan dari ibu akan disalurkan ke bayi melalui umbilical vein. bahan-bahan buangan daripada bayi pula akan disalur ke ibu melalui umbilical artery. tetapi, dalam TRAP, si A punya bahan buangan disalurkan kepada si B. jadi, si B yang sepatutnya mati dapat juga merasa sisa-sisa makanan daripada si A dan menyebabkan dia membesar tanpa struktur yang sebenar. si B tiada kepala, otak, tangan, jantung. Maka, orang-orang terdahulu pun memberikan nama A sebagai "pump" atau si pengepam dan B sebagai "acardiac" atau si tiada jantung. Dapat dilihat di sini bahawasanya, si pengepam (A) berusaha keras untuk membekalkan makanan kepada kembarnya yang tiada jantung itu. Ini menyebabkan, jantung A terbeban dengan kerja tambahan dan berisiko untuk mendapat 'cardiac failure' (kegagalan jantung) semasa lahir nanti.
fenomena luar biasa ini sebenarnya telah terjadi beberapa kali di Malaysia ini. Namun, oleh sebab saya ni kurang prihatin dengan masalah-masalah seperti ini sehinggalah memasuki posting OnG baru berminat untuk tahu.
boleh la klik di bawah ini untuk 'more info':
1. http://www.sinarharian.com.my/perak/content/story6060462.asp
2. http://www.indianpediatrics.net/july2003/july-683-684.htm
3. http://www.centrus.com.br/DiplomaFMF/SeriesFMF/11-14weeks/chapter-05/chapter-05-final.htm
have you ever heard about TRAP-twin reversed arterial perfusion? it is a condition occurs in twin pregnancy where one twin supplies blood and nutrition to the other twin which is already dead.
this was the first time i heard about the phenomenon.
emm...kalau dalam bahasa melayu mungkin dipanggil "kembar pengepam darah". kes ni berlaku 1 dalam 35000 pregnancies. dan yang satu tu pernah ada di wad kuning dekat sini.
kisahnya macam ni...
TRAP ni ialah satu komplikasi yang sangatlah jarang berlaku di kalangan ibu yang mengandung kembar. ia melibatkan satu kembar yang ada kecatatan dari segi struktur dan tidak boleh survive manakala kembar yang satu lagi adalah normal dan bertindak sebagai pembekal darah dan makanan kepada pasangan kembarnya tu.
nak tahu lebih lanjut, boleh la google2. macam2 ada.

Ini nak menunjukkan bagaimana TRAP terjadi. darah dan makanan dari ibu akan disalurkan ke bayi melalui umbilical vein. bahan-bahan buangan daripada bayi pula akan disalur ke ibu melalui umbilical artery. tetapi, dalam TRAP, si A punya bahan buangan disalurkan kepada si B. jadi, si B yang sepatutnya mati dapat juga merasa sisa-sisa makanan daripada si A dan menyebabkan dia membesar tanpa struktur yang sebenar. si B tiada kepala, otak, tangan, jantung. Maka, orang-orang terdahulu pun memberikan nama A sebagai "pump" atau si pengepam dan B sebagai "acardiac" atau si tiada jantung. Dapat dilihat di sini bahawasanya, si pengepam (A) berusaha keras untuk membekalkan makanan kepada kembarnya yang tiada jantung itu. Ini menyebabkan, jantung A terbeban dengan kerja tambahan dan berisiko untuk mendapat 'cardiac failure' (kegagalan jantung) semasa lahir nanti.
fenomena luar biasa ini sebenarnya telah terjadi beberapa kali di Malaysia ini. Namun, oleh sebab saya ni kurang prihatin dengan masalah-masalah seperti ini sehinggalah memasuki posting OnG baru berminat untuk tahu.
boleh la klik di bawah ini untuk 'more info':
1. http://www.sinarharian.com.my/perak/content/story6060462.asp
2. http://www.indianpediatrics.net/july2003/july-683-684.htm
3. http://www.centrus.com.br/DiplomaFMF/SeriesFMF/11-14weeks/chapter-05/chapter-05-final.htm